Has a patient ever complained of nonspecific posterior shoulder pain (usually in the overhead position)? There also may be a painful popping and a sense of looseness in the shoulder, and some positive impingement signs.1 If so, you could be dealing with a SLAP (superior labrum, anterior to posterior) lesion. The glenoid labrum is a fibrous rim that attaches to the periphery of the glenoid fossa and helps to deepen it, thereby increasing the surface area of the glenoid. This deepening helps stabilize the humeral head - especially in the midrange of glenohumeral motion, at which point the ligamentous capsular structures are lax.2 The labrum also serves as an attachment for the glenohumeral ligaments.
A SLAP lesion originates at the superior posterior labrum to the biceps anchor and extends anteriorly on the superior labrum. The proximal biceps tendon originates from the supraglenoid tubercle of the glenoid and blends into the fibers of the labrum and capsule surrounding this insertion. With type 1 and type 3 SLAP lesions, the biceps attachment to the labrum is intact; with type 2 SLAP and other such lesions, the biceps are pulled away from the glenoid attachment. This lack of a firm attachment of the biceps to the glenoid results in glenohumeral instability. Therefore, a labral injury may occur without biceps involvement, especially when the injury is of the compression type, such as those that occur as the result of a fall or repetitive compression from overhead throwing.3
The common type 2 SLAP lesion, in which the biceps tendon is detached, is usually a traction-type injury by which the biceps causes an avulsion of the superior labrum (deceleration phase of throwing). The patient also may complain of biceps tendinopathy, popping and clicking, due to the torn labrum. The superior laxity created by the loss of the biceps insertion may lead to damage to the posterosuperior porton of the rotator cuff, which may be associated with chronic SLAP problems. Rotator cuff injuries are not usually found in acute SLAP lesions.3 It appears that shoulder instability may stress the biceps insertion, leading to biceps detachment, or biceps detachment may lead to shoulder instability. Since the biceps tendon helps resist anterior translation, and supports the inferior glenohumeral ligament when the shoulder is in abduction and external rotation (cocking phase of the throw), if the shoulder is already unstable, the biceps are forced to overwork by increasing its protective compressive force, causing increased stress to the superior labrum and biceps tendon complex.
It has been proven that abduction and external rotation of the shoulder during the cocking phase of throwing stresses the origin of the long head of the biceps tendon, and its attachment to the posterior labrum.4
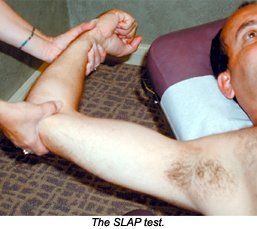
Kim, et al.,5 created a test for SLAP lesions that was positive mostly for the type Z lesion. The biceps load test II had a sensitivity of 89.7 percent; a specificity of 96.9 percent; a positive-predictive value of 92.1 percent; a negative-predictive value of 95.5 percent; and a kappa coefficient of 0.815. The test is performed as follows: The supine patient's arm is elevated to 120¡ and externally rotated to its maximal point, with the elbow in the 90¡ flexed position and the forearm in the supinated position. The patient is asked to flex the elbow while being resisted by the examiner. This is the position that reproduces the mechanism in the development of type 2 SLAP lesions.
Forceful traction of the displaced biceps-superior labral complex occurs during the active contraction of the biceps muscle against resistance. Kim, et al., believe the test position changes the relative direction of the biceps fiber in a position of an oblique angle to the posterosuperior labrum, causing a peeling of the superior labrum off the glenoid margin.
The test is positive if the patient complains of pain during resisted elbow flexion, or if the patient complains of more pain from the test than the pain that was already present in the test position. The test is negative if pain is not elicited by resisted elbow flexion, or if the pre-existing pain is unchanged or diminished by resisted flexion.
References
Kim S-H, Ha KK-I, Han K-Y. Biceps load test: a clinical test for superior labrum anterior and posterior lesions in shoulders with recurrent anterior dislocations. Amer J Sports Med 1999; 27(3):300-307.
Lippett FG. A modification of the gravity method of reducing anterior shoulder dislocations. Clin Orthop 1982; 165:259-260.
Maffet MW, Lowe WR. Superior labral injuries. In: DeLee JC, Drez D. Orthopaedic Sports Medicine, Vol 1. Philadelphia: Saunders;2003.p.1046-1064.
Rodosky MW, Harner CH, Fu FH. The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J sports Med 1994;22:121-130.
Kim S-H, et al. Biceps load test II: a clinical test for slap lesions of the shoulder. Arthroscopy: The Journal of Arthroscopic and Related Surgery 2001;17(2):160-164.
Many relevant diagnostic signs are not performed deliberately by the examiner or by the patient at the examiner’s direction. They are observed as the patient reacts to their condition. Fortin’s finger sign, Minor’s sign, and Vanzetti’s sign are three examples of this principle.
Spearheaded by burgeoning scientific and clinical research literature, psychedelics have reached a level of media coverage and popular interest that has not been seen for over half a century. By “psychedelics,” we are referring to the unique class of substances that includes psilocybin (the active compound found in so-called “magic mushrooms”), LSD, dimethyltryptamine (DMT), ayahuasca, 5-MeO-DMT, and mescaline – each of which occurs in the natural world (except for LSD, which is a semi-synthetic compound).
While working at the Lovelace Medical Center in Albuquerque, N.M., one of the primary care physicians stated that imaging every patient prior to receiving chiropractic was not medically necessary. It was at that point I reconsidered the need for the imaging of every patient to avoid malpractice.