The Importance of Proprioceptive Testing to Chiropractic
Scott Cuthbert, DC
For about 76 million Americans, proprioceptive disorders cause more than a passing problem. More than 5 million of them visit their doctors each year because occasional or chronic feelings of wooziness, spinning, lack of balance, and fainting are seriously interfering with their ability to work or to enjoy their leisure. In fact, dizziness and other equilibrium disorders are among the most common symptoms reported to physicians.1
Proprioceptive testing should be performed on any patient who complains of disturbed balance, or if there is a suspicion that equilibrium disturbances exist in the patient. Because postural and proprioceptive functions are so automatic, they are often taken for granted, even in the clinical setting. If the patient walks onto the examination table, the doctor then looks for pain and its cause. But the cause of the problem may be discovered only when testing the patient while proprioception is going on, or while the patient is moving.
This tendency toward lack of awareness of the proprioceptive integrity in our patients is especially true if only a mild dysfunction exists that does not obviously interfere with gait and stability during locomotion. One of the more difficult tasks facing the physician is to recognize not only the existence, but also the significance of slightly disordered postural mechanisms.
Since equilibrium reactions are subtle, sometimes even virtually unobservable when they involve little or no motion, eliciting them and observing their response require special skill. It is particularly easy to overlook the importance of equilibrium reactions in the supine or prone position.
Arguments for activating postural mechanisms in our patients in the prone, supine, sitting, standing and moving positions have been given elsewhere in the AK literature (PRYT testing, Freeman-Wyke one-leg-standing testing, eyes-into-distortion, body-into-distortion, ocular lock, oculo-basic, gait testing, etc.).2-5 The examination for postural hypotension, or Ragland's sign (a common side-effect of adrenal stress disorder), is also a part of every applied kinesiology initial examination.
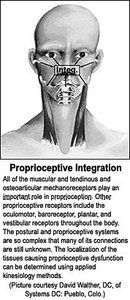
Sherrington derived the term proprioception (1906) from the Latin proprius, to refer to the organism's perception of sensations that originate in receptors that are stimulated by its own movement. Sherrington identified the muscle spindles, mechanoreceptors in joints, and vestibular receptors as the primary sources of proprioceptive inputs.6
Sherrington, Guyton,7 and many other neurophysiologists also have identified the many sensory receptors (mechanoreceptor, vestibular, visual, muscle spindle, Golgi tendon organ, ligaments and tendons and their associated capsules and sheaths) as the sources of "proprioceptive inputs" into the nervous system. The mechanoreceptors feed into the nervous system information about movement, tension and pressure. The mechanoreceptors are present in all vertebrates and in all tissues in which active or passive movements occur. These include the skeletal muscles, bones, joints, ligaments and tendons and their associated capsules and sheaths; the skin; the internal ear; the eyes; the digestive tract; the respiratory, cardiovascular and genitourinary system.
A single event (such as pain signals arising from damaged tissue) can have widespread influence throughout the rest of the nervous system, and the consequences of the reaction to that event can cascade through many levels of function and behavior.8 Clinically, we find that even though the tissue injury may have been to a small area, it is possible to observe changes throughout the body.
Body posture and balance can be adversely influenced by dysfunctions affecting the central nervous system, the peripheral nervous system, the eyes, the ears, and the musculoskeletal system, where proprioceptor and mechanoreceptor sensory organs lie. Defects in any of these tissues can lead to diminished postural function and increased instability, and eventually to trauma from falling. There is evidence that multiple factors can adversely affect the postural mechanism and that these factors are cumulative.9 One of the causes of the chiropractic subluxation may be found in faulty proprioceptive mechanisms in our patients. Proprioception, equilibrium and balance are at the core of human functioning.
For voluntary movements to be well-timed, accurate and painless, they require coordinated tactile, visual and proprioceptive information about the movement in progress. Locomotion should be a stable cycle generated by sensory links between the musculoskeletal system, the nervous system and the environment.10 Without adequate sensation, ongoing function is limited and poorly controlled. Voluntary movement depends upon integration of the motor and sensory systems. Manual muscle testing allows a physician to evaluate this interaction with a method distinctly tailored to monitor precisely this. Sensory information is necessary for the control of movement and is used to correct errors through feedback and feed-forward mechanisms.11 Any problem or confusion within the sensory system may affect the guidance systems for movement, leading to inefficient muscular activity for any task required.
It is well-accepted that alterations in the function of the sensory system may impede postural stability. For example, distortions in the proprioceptive information from diseased joints, such as an arthritic knee or spondylitic vertebrae, will affect the individual's perception of position.12 Diseases affecting cutaneous afferent fibers, such as in diabetic neuropathy, may interfere with information about motion coming from the soles of the feet.13 It is an accepted biological fact that appropriate muscle tone and tension are necessary for skeletal structures to be stable, and any condition that alters the tone of the muscles leads to instability in the structure during activity. Faults can appear at any level of the controlling system of muscles - on the sensory, the integrative, or the motor side.
It is no longer appropriate to think of isolated sensory modalities in relation to proprioceptive function. That is not the way the brain functions. It functions as a whole. This point is emphasized because applied kinesiology theory believes that to resolve biomechanical, locomotor, postural and sensory problems, many areas of the body must be examined and corrected in order to achieve long-lasting symptomatic relief. Our global view of integrated biomechanics and neurophysiology is one of the major differences between chiropractic (and especially applied kinesiology) and many of the other manipulative and medical professions.
Our objective in treating proprioceptive disorders is to increase the brain's capacity to integrate proprioceptive sensation from the body's receptors by developing the motor responses that aid this mechanism. This will allow the patient to gradually self-induce proprioceptive stimulation, thereby potentiating this portion of the sensory system on a daily basis.
Many of these proprioceptive receptors (mechanoreceptors, but also muscle spindles, visual righting reflexes, the positive support mechanism in the feet, etc.) are embedded in the muscles and connective tissues surrounding the joints of the body, and it is thought within applied kinesiology that alteration in muscle or connective tissue tone (myofascial dysfunction) may interfere with these feedback mechanisms.
Treatment that leads to better processing of information at the sensory receptor, spinal cord, or a higher level, should also reduce the neural consequences of proprioceptive dysfunction. Normalizing tissue tone, signaling and circulation should help normalize signals that are entering the nervous system, and thus gradually allow the nervous system to shift back to normal.
The interrelationships between proprioceptive testing and treatment, equilibrium and postural problems, the chiropractic subluxation, hypotonicity on manual muscle testing, cranial faults and other related factors found on AK evaluation may seem complex and tangled, but they are all causative factors that must be recognized and managed in our problem patients.
References
Alexander, N B. Postural control in older adults. Journal of the American Geriatric Society, 1994:42;93-108.
Sherrington, Charles S. The Integrative Action of the Nervous System. New Haven: Yale University Press, 1906.
Guyton, A.C. Textbook of Medical Physiology. Philadelphia, PA: W.B. Saunders, 1991.
Lund JP, et al. The pain-adaptation model: a discussion of the relationship between chronic musculoskeletal pain and motor activity. Canadian Journal of Physiology and Pharmacology, 69, 683-694, 1991.
Wolfson, L., Whipple, R, Derby, C A et al. A dynamic posturography study of balance in health elderly. Neurology 1992;42:2069-2075.
Winter, D.A., et al. Assessment of balance control in humans. Medical Progress through Technology: 16; 31-51, 1990.
McCloskey, D.I., Prochazka, A. The role of sensory information in the guidance of voluntary movement. Somatosensory and Motor Research:11; 69-76,1994.
Barrett, D. S, Cobb, A G, Bentley, G. Joint proprioception in normal, osteoarthritic and replaced knees. Journal of Bone and Joint Surgery, 1991;73:53-56
Simoneau, G.G., et al. Postural instability in patients with diabetic sensory neuropathy. Diabetes Care 17:1411-1421, 1994.
Building on a historic March 2026 meeting between Make America Healthy Again and chiropractic leadership, MAHA has announced the launch of the MAHA Chiropractic Hub, “a coordinated national partnership uniting MAHA Center, MAHA Action, and the chiropractic profession, including national associations, state organizations, practitioners, educators, researchers, and patient advocates. The Chiropractic Hub will advance federal policy, expand patient access, and build broad public support for chiropractic care across America.”
The chiropractic profession is confronting one of the most significant federal regulatory threats it has faced in decades. A new U.S. Department of Education (ED) accountability framework – commonly referred to as the “Do No Harm” (DNH) regulation – could place many chiropractic programs at risk of losing access to federal financial aid (student loans), potentially reshaping the future of chiropractic education and workforce development across the United States.
Pain has become the dominant language of musculoskeletal healthcare. Numeric pain-rating scales and symptom reports are routinely used as primary indicators of clinical success. But while pain reduction is meaningful, it is an incomplete and often misleading representation of recovery. This has real consequences for patient adherence, long-term outcomes, and how conservative care is perceived within the broader healthcare system.