A seldom attended articulation in the shoulder girdle is the first rib. We motion palpate the heck out of the glenohumeral joint; some of us actually motion palpate the scapula. But how many of us consider the first rib as part of the shoulder girdle? We should.
When the patient has that persistent, nagging, "shoulder pain," that "something not right in the shoulder," the "almost better but ..." shoulder, the "tingling down the arm" shoulder, it is way past time to evaluate the first rib.
What I have found in clinical practice (descriptive research) is that there is a reliable specific sequence to locate, evaluate, and adjust the first rib.
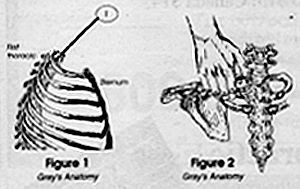
Where Is the First Rib?
Before you can palpate (either static or motion) the first rib you have to know where it is located.
How to Get There ...
Standing behind the patient, place your thumb in front of the trapezius pointing posterior medial with your fingers curled about the clavicle. The suggestion of curling your fingers about the clavicle is to prevent your fingers from resting on the pectoralis muscles, possibly making the patient feel compromised.
There are two methods that I know of:
Rotate and lateral flex the head to the opposite side you are evaluating. This brings the rib head (costotransverse and facet) closer to the surface. But it causes the trapezius, levator scapulae, and scalenus anticus muscles to become taut.
Rotate and lateral flex the head toward the side you are evaluating. This causes the rib to go slightly from the surface. However, as the head is rotated and lateral flexed the musculature creates a "pocket," an invagination, an indentation.
I prefer the later simply because when you follow the pocket in with your thumb as it is being formed by rotating and lateral flexing the head, you will be "directed" to the first rib. Challenge the first rib with a light springing of the articulation. If the problem is the first rib, it will be very, very tender to the patient.
Caution
I will have to assume here that when you challenge the rib that your contact is NOT on the carotid artery and/or any portion of the brachial plexus.
Now That I Can Find It, What Do I Do with It?
Move it, of course! I have found that the first rib needs to be "re-seated" into the facet and "re-introduced" to the anterior portion of the transverse process.
Whatever technique you choose to adjust the first rib, make sure you recheck to confirm or deny your adjustment. A word of descriptive research here: If the first rib has been subluxated for any length of time, it will be very, very tender.
Summary
Be aware of the possibility of a first rib subluxation in patients with headaches, shoulder pain, carpal tunnel syndrome, chest pain, neck pain, rhomboid pain, upper and middle thoracic pain, elbow, wrist, and hand pain, etc.
I hope that the above has helped you in your first rib -- specific adjusting. Write me to let me know if I am right in my clinical approach.
Charles Rollis, BS, DC 826 N. Winchester Blvd. Suite 2-D San Jose, CA 95128 Fax: (408) 246-4299
Many relevant diagnostic signs are not performed deliberately by the examiner or by the patient at the examiner’s direction. They are observed as the patient reacts to their condition. Fortin’s finger sign, Minor’s sign, and Vanzetti’s sign are three examples of this principle.
Spearheaded by burgeoning scientific and clinical research literature, psychedelics have reached a level of media coverage and popular interest that has not been seen for over half a century. By “psychedelics,” we are referring to the unique class of substances that includes psilocybin (the active compound found in so-called “magic mushrooms”), LSD, dimethyltryptamine (DMT), ayahuasca, 5-MeO-DMT, and mescaline – each of which occurs in the natural world (except for LSD, which is a semi-synthetic compound).
While working at the Lovelace Medical Center in Albuquerque, N.M., one of the primary care physicians stated that imaging every patient prior to receiving chiropractic was not medically necessary. It was at that point I reconsidered the need for the imaging of every patient to avoid malpractice.