Isthmic vs. Degenerative Spondylolisthesis: Using the "Wide Canal Sign"
Deborah Pate, DC, DACBR
Spondylolisthesis is generally defined as the anterior shift of one vertebral body on another (the segment below it). It is a well-recognized disorder that can cause lower back pain and radiculopathy. Two of the more common causes for a spondylolisthesis are degenerative joint disease of the lumbar facets, allowing anterior slippage of the vertebral body in relation to the one below; and a defect in the pars interarticularis.
Generally, oblique views are performed to visualize the pars interarticularis if there is a spondylolisthesis. Sometimes, however, the oblique view is not helpful because of marked degenerative facet changes that obscure the pars. The cause of the spondylolisthesis needs to be determined because the clinical management will be different, depending on the cause.
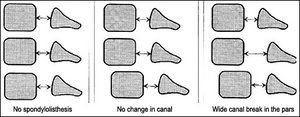
By using the simple anatomic concept that a spondylolisthesis associated with a break in the pars will demonstrate an increase in the sagittal diameter of the spinal canal, the two etiologies can be differentiated. Using the lateral view, determine the diameter of the spinal canal. A simple method is to use the middle of the posterior margin of the vertebral body and the spino-laminar junction as an estimate of the spinal canal, and compare the level with the spondylolisthesis and the adjacent levels. If there is no significant change in the measurement, it is unlikely that a pars defect is causing the spondylolisthesis (see figure above).
This concept is just a guide for determining if there is a lysis of the pars. Further imaging may be necessary to determine if there are other complications, particularly with marked degenerative changes.
Just as a caveat, there is an additional test you can use to determine whether there is anterior spondylolisthesis. This is the right-angle test. An angle is drawn perpendicular to the anterior margin of the sacrum and along the superior margin of the sacrum (see example below).
Many relevant diagnostic signs are not performed deliberately by the examiner or by the patient at the examiner’s direction. They are observed as the patient reacts to their condition. Fortin’s finger sign, Minor’s sign, and Vanzetti’s sign are three examples of this principle.
On Feb. 1, 2024, two more legislators – John R. Carter (R-Texas) and Robert “Bob” Good (R-Va.) – co-sponsored the Chiropractic Medicare Coverage Modernization Act of 2023, bringing the co-sponsor total to 155, two more than the total achieved over the entire two-year congressional cycle in which identical legislation last appeared (2021-22).
While working at the Lovelace Medical Center in Albuquerque, N.M., one of the primary care physicians stated that imaging every patient prior to receiving chiropractic was not medically necessary. It was at that point I reconsidered the need for the imaging of every patient to avoid malpractice.