Chiropractic Care in the Third Trimester of Pregnancy: Evaluation of In Utero Constraint
Judy A. Forrester
Editor's note: Dr. Judy Forrester graduated from CMCC in 1978 with the "President's Graduate of the Year" award and is a practitioner in Calgary, Alberta, Canada, specializing in prenatal, perinatal and neonatal care. As co-founder of the Peter Pan Potential, an educational organization for the teaching and promotion of chiropractic pediatric care and research, and an international National Speakers' Association lecturer for a diversity of continuing education programs, including the Life Chiropractic College Pediatric Diplomate Program, Dr. Forrester travels extensively to foster academic and clinical knowledge in her specialty. She is a contributing author in her specialty of prenatal and perinatal care to the Pediatric Chiropractic Textbook, due to be published by Williams and Wilkins this year, and was highlighted in the Chiropractic Centennial Documentary.
This is a slightly different version of Dr. Forrester's article that first appeared in the Canadian Chiropractor magazine (Vol. 1, issue no. 2, 1996, p. 36). Further inquiries may be addressed to the Canadian Chiropractor, 31 Abbott Ave., Toronto, ON M6P 1H3.
The third trimester of pregnancy, commencing at seven months gestational age, heralds the perinatal period. This critical period is the greatest concern to obstetricians, physicians and midwives due to the propensity for adversity in the fetal presentation, position and attitude. The biomechanical implications affecting fetal well-being during the last trimester, and for the preparatory phase for labour and delivery, embrace any fetal alignment other than the optimal longitudinal lie, vertex presentation, and flexion attitude. Distinctly, the doctor of chiropractic may play an intrinsic role in the evaluation of in utero constraint, which describes the biomechanical premise for neuromusculoskeletal compromise of fetal well-being. Additionally, the opportunity to positively influence the pelvic and uterine environment from a chiropractic perspective is significant to fetal outcome relevant to the description of in utero constraint.
Table 1: Fetopelvic Relationships According to Fetal Position
Presentation
Longitudinal lie (99.5%)
Cephalic (96-97%)
Breech (3-4%) Complete
Frank
Footling: single, double Kneeling: single, double Transverse or oblique lie (0.5%) Shoulder
Vertex (posterior part) Vertex (median part) Brow Face
Buttocks
Buttocks
Knees
Knees
Shoulder, arm trunk
Denominator
Occiput (O)
Occiput (O)
Forehead (frontum) (Fr) Chin (mentum) (M)
Sacrum (S)
Sacrum (S)
Sacrum (S)
Sacrum (S)
Sacpula (Sc)
The obstetrical terms describing fetopelvic relationships are of significance to the doctor of chiropractic working with the third trimester maternity patient. (Table 1). Fetal lie refers to the relationship of the long axis of the fetus to the long axis of the mother. The two lies are: (1) longitudinal, where the long axis of the fetus and mother are parallel; and (2) transverse, or oblique, when the long axis of the fetus is perpendicular or oblique to the long axis of the mother when she is in an upright position. (Table 1). These lies are divided into fetal presentations which specify the part of the fetus lying over the pelvic inlet or cervix. The primary presentations are (1) cephalic or vertex, when the fetal head emerges first; and (2) breech, when the buttocks or lower extremities present at the introitus.
The presenting part is illustrated as the most dependent part of the fetus, lying nearest the cervix. The denominator is an arbitrarily chosen point on the presenting part of the fetus used in describing position. Each presentation has its own denominator.
Obstetrical position describes the relationship of the denominator to the anterior, posterior or lateral aspects of the maternal pelvis. The denominator can occupy any part of the 360 degree circumference of the pelvic girdle. Fetal position may be described as anterior, posterior, or transverse, depending upon which side of the maternal pelvis the denominator is in. Fetal attitude relates the fetal parts to each other. The basic attitudes are flexion and extension. The fetal head is in flexion when the chin approaches the chest and in extension when the occiput nears the spine. The typical fetal attitude in the uterus is flexion, with the head bent in front of the chest, the arms and legs folded in front of the body, and the back curved forward slightly.
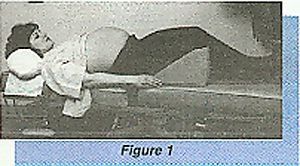
Palpation of the fetal structures to assess fetopelvic relationships is accomplished with expertise within the chiropractic arena. A variation of Leopold's maneuvers is recommended for this purpose. To examine the third trimester patient, she should be instructed to lie on her back with the abdomen exposed (Fig. 1). In order to facilitate relaxation of the abdominal wall muscles, the shoulders should be raised slightly and the knees are up and comfortable. If the patient is in labour, the examination can be easily performed between contractions.
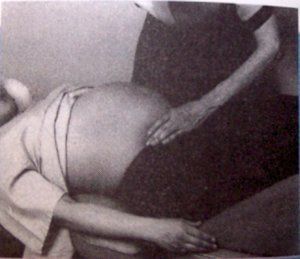
The first maneuver is designed to determine the presenting fetal part. The chiropractor should stand at the patient's side and gently, but firmly grasp the lower uterine segment between the thumb and fingers of the inferior hand to palpate the presenting part (Fig 2). The superior hand should then be placed on the fundus to steady the uterus and apply slight counter pressure. This maneuver is best performed initially, as the head is the part of the fetus that can be identified with the most certainty. It is palpated as hard, round and regular-shaped, and is very easily ballottable when it is located in the uterine fundus. It is occasionally possible to palpate the neck as a furrowed structure, however, the depth at which the baby is positioned may make it more difficult to ascertain. It is usually a simple procedure to align the glabella under one of the examining fingers and the external occipital protuberance under the other; this facilitates the examiner in moving the fetal head. The fetal head can also be pushed posteriorly in the pelvic cavity, where the amniotic fluid buoys the head. When this type of pressure on the fetal head is released, the head rises back and abuts against the examiner's hand or fingers.
Since the fetal head is at or in the pelvis in over 90 percent of pregnancies, the rational thing to do first is to look for the had in its most frequent location. When it has been confirmed that the fetal head is at the inlet, two important facts are discovered. Chiefly, that the lie is longitudinal, and that the presentation is cephalic.
An attempt should be made to gently maneuver the head from side to side to see whether it is still outside the pelvis and floating, or in the pelvis and fixed or engaged.
Secondly, with the inferior examining hand applied to the presenting apart, the superior examining hand palpates the uterine fundus (Fig. 3). The breech is most often located here and feels softer, more irregular, less globular and less like a defined structure than the head. It is not as easily moveable as the head and is continuous with the spinal column. When it is attempted to ballot the breech, the body moves laterally with it. A description by the mother of fetal movement such as kicking and pummeling assists in diagnostic confirmation. Moreover, palpation of mobile, small parts in the proximity of the breech aids in detection.
This step is sequentially significant, because a comparison can be made between the fetal structures perceived in a longitudinal lie by the simultaneous palpations of the two examining hands. Both hands may palpate a suspected structure at either the fundus or the pelvic inlet in the course of evaluation. This process assists in the positive confirmation of the presenting part.
The third maneuver to be performed is to confirm the location of the fetal spinal column. This is best accomplished by placing the hands on either side of the abdomen (Fig 4). It is best if one hand is employed to feel the fetus while the other assists in securing the uterus. The fetal spine is perceived as firmer, smoother and somewhat rigid. It should form a gradual convex arch, and as pressure is applied toward the maternal umbilicus, there is uniform resistance to the palpating fingers.
On the contralateral side, there is uneven resistance to examining pressure, with the fingers burrowing more deeply in some areas than in others. Any palpation of moving appendages facilitates diagnosis.
The fourth maneuver concludes the abdominal examination by locating the cephalic prominence. The cephalic prominence can be palpated through the abdomen by placing both hands on the sides of the lower part of the uterus with the fingers aligned inferiorly, and moving gently toward the pubis (Fig. 5). When there is a cephalic prominence, the examining fingers abut against it on that side, and on the contralateral side meet with little or no resistance. The location of the cephalic prominence aids in diagnosing attitude.
The cephalic prominence is produced by flexion or extension of the fetal head upon the neck. When the fetal head is well flexed, the occiput is lower than the sinciput and the forehead is the cephalic prominence. When there is extension, the occiput is higher than the sinciput and the occiput is the cephalic prominence. When the cephalic prominence and the spine are on opposite sides, the attitude is termed as flexion. When the cephalic prominence and the spine are on the same side, the attitude is that of extension. When no cephalic prominence is palpable, there is neither flexion nor extension and the head is in a neutral position, known as the military attitude.
When determination of the fetopelvic relationship has been rendered, the responsibility for alteration of any adversity causing biomechanical implications to the fetus can then move into the chiropractor's clinical arena of correction of maternal pelvic biomechanical insult. Gentle and specific soft tissue and articular techniques including those affecting the lumbosacral spine, pelvic outlet and pelvic cavity may be applied to encourage a normal fetopelvic relationship. Additionally, fetal version techniques specific to the scope of chiropractic practice can be effectively and safely employed. These techniques will be described in a future article. The optimal outcome of chiropractic practice in this domain can promote the efficacy of a safe and non-intervened birth process, and ultimately a healthy neonate.
Judy A. Forrester, DC Calgary, Alberta Canada (403) 247-2947
Spearheaded by burgeoning scientific and clinical research literature, psychedelics have reached a level of media coverage and popular interest that has not been seen for over half a century. By “psychedelics,” we are referring to the unique class of substances that includes psilocybin (the active compound found in so-called “magic mushrooms”), LSD, dimethyltryptamine (DMT), ayahuasca, 5-MeO-DMT, and mescaline – each of which occurs in the natural world (except for LSD, which is a semi-synthetic compound).
At its March 11, 2024, meeting, the Council for Higher Education Accreditation (CHEA) Committee on Recognition reviewed the formal request for a change in the CHEA-recognized scope of accreditation submitted by the Council on Chiropractic Education (CCE). The new CHEA-approved scope statement is: “The Council on Chiropractic Education accredits doctor of chiropractic degree programs and chiropractic residency programs in the United States, its territories and Canada (2024).”
Many relevant diagnostic signs are not performed deliberately by the examiner or by the patient at the examiner’s direction. They are observed as the patient reacts to their condition. Fortin’s finger sign, Minor’s sign, and Vanzetti’s sign are three examples of this principle.